News
Advertisement
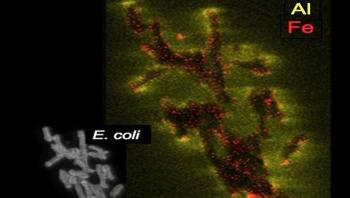
Since prehistoric times, clays have been used by people for medicinal purposes. Whether by eating it, soaking in a mud bath, or using it to stop bleeding from wounds, clay has long been part of keeping humans healthy. Certain clays have also been found with germ-killing abilities, but how these work has remained unclear. A new discovery by Arizona State University scientists shows exactly how two specific metallic elements in the right kinds of clay can kill troublesome bacteria that infect humans and animals.
Advertisement
Q: Recently our facility was cited for disinfected laryngoscope blades that were found unprotected from re-contamination in storage. What is the recommended practice for these items?A: This question has many implications. CDC’s Healthcare Infection Control Practices Advisory Committee (HICPAC) says laryngoscope blades are “semicritical” items, which are defined as, “Items that directly or indirectly contact mucous membranes of the respiratory tract. They should be sterilized or subjected to high-level disinfection before reuse.” After they are cleaned according to the manufacturer’s IFU, there are several options for processing laryngoscope handles and blades. Many laryngoscope blades can be high-level-disinfected. If high-level disinfection is used (check the manufacturer’s IFU for compatible chemicals), the blade must be protected from recontamination after processing. One way of accomplishing this is to place the blade in a zip-lock bag and then apply a “Clean Not Sterile” label to the top of the bag. (Make sure that you clean your hands first.) If anyone opens the bag, the label will be damaged indicating the blade could be contaminated. At some facilities, laryngoscope blades are sterilized, which is acceptable but not necessary (CDC, 2003). Packaging blades requires the package to be opened if nursing must test the laryngoscope bulb on the blade. This results in a blade being replaced inside an open paper-plastic pouch. The opened pouch does not protect the blade from contaminates.
Advertisement

So much of the infection preventionist’s time has traditionally been spent in the pursuit of healthcare personnel education and training on infection control-related principles and practices, with varying degrees of success measured through compliance metrics. Be it hand hygiene compliance percentages, terminal cleaning effectiveness rates, or various infection prevention bundles, compliance can be suboptimal in many healthcare institutions - and healthcare workers freely admit it. For example, Yassi, et al. (2007) assessed the determinants of healthcare worker self-reported compliance with infection control procedures via a survey of personnel in 16 healthcare facilities. A strong correlation was found between both environmental and organizational factors and self-reported compliance; no relationship was found with individual factors. The researchers found that only 5 percent of survey respondents rated their training in infection control as excellent, and 30 percent felt they were not offered the necessary training. The investigators concluded that compliance with infection control procedures is tied to environmental factors and organizational characteristics, suggesting that efforts to improve availability of equipment and promote a safety culture are key. They added that training should be offered to high-risk personnel, demonstrating an organizational commitment to their safety. We spoke with Sue Barnes, RN, CIC, the national leader of infection prevention and control in the Program Office for Kaiser Permanente in California, for her perspective on issues relating to boosting compliance with infection prevention and control imperatives, and what clinical issues are driving interventions.
Advertisement

Healthcare-acquired infections (HAIs) continue to be a challenge for healthcare professionals today. Despite increased attention to infection control protocol and increased focus on personal protection there has not been any sustainable reductions in the spread of infection. This leaves healthcare workers, patients and the general public continually at risk.

The global supply of oral cholera vaccines (OCV) is set to double after the World Health Organization (WHO) approved a third producer, helping to address global shortages and expand access in more countries. Globally, OCV production is low, with demands currently exceeding supply. Sudan and Haiti last year made requests to WHO for supplies of vaccines to conduct pre-emptive vaccination campaigns that could not be filled because of the global shortage.

When the Ebola virus outbreak erupted in West Africa in 2014, children infected with the virus -- particularly those under age 5 -- faced overwhelming challenges. Not only was there a high death rate among young children infected with the disease, they often were isolated from their families, leaving them feeling distressed and without the intensive care they needed.

Researchers at the Skaggs School of Pharmacy and Pharmaceutical Sciences at the University of California, San Diego have entered into a research collaboration with Janssen Research & Development, LLC (Janssen R&D), one of the Janssen Pharmaceutical Companies of Johnson & Johnson, to identify new therapeutic targets for Chagas disease, a parasitic infection that is the leading cause of heart failure in Latin America.

New research from North Carolina State University and the University of Michigan finds that bile acids which are altered by bacteria normally living in the large intestine inhibit the growth of Clostridium difficile, or C. diff. C. diff is a harmful bacterium that can cause painful and sometimes fatal infections. The work sheds light on the ways in which some commonly used antibiotics can promote C. diff infections by killing off the bile acid-altering microbes.
Research from the Johns Hopkins University Applied Physics Laboratory (APL) in Laurel, Md., into better methods of predicting outbreaks of the mosquito-borne dengue virus was selected for presentation in September at the Eisenhower Executive Office Building - part of the White House complex. The APL team had developed new options for forecasting the spread of dengue fever, which affects up to an estimated 390 million people annually worldwide.
Advertisement
Advertisement