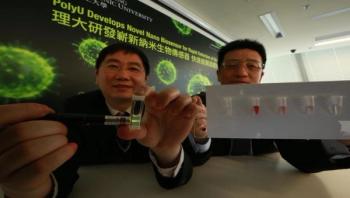
PolyU's new invention utilizes an optical method called upconversion luminescence resonance energy transfer (LRET) process for ultrasensitive virus detection. It involves simple operational procedures, significantly reducing its testing duration from around one to three days to two to three hours, making it more than 10 times quicker than traditional clinical methods. Its cost is around HK$20 per sample, which is 80 percent lower than traditional testing methods. The technology can be widely used for the detection of different types of viruses, shedding new light on the development of low-cost, rapid and ultrasensitive detection of different viruses.